We get called out to this 62yo lady complaining of weakness and nausea, 12 looked okay for the 7-10 mins max on scene (got history from her and husband, she had some tricky corners in the house lol) but as soon as we load her in the unit, she had runs of this every 30 secs or so, lost consciousness twice on us an 8 min transport. The run of that rhythm itself would typically resolve/stop after about 10-15 seconds, then come on again, stop, then start. When she’d lose consciousness it was super sudden, and her head would start to fall back or forward and she’d snap awake about 5-10 seconds later. Everytime she lost consciousness it was following a run of that rhythm on the monitor. During her first run (im referring to the first few secs or so on lead 2+3, the “run” in referring to would cease and return to what the second half of the strip looks like) my medic had me put the pads on as a “just in case” and had me just start driving at that point as he was mostly finished getting his access by that point as well. My medic calls report, then the loss of consciousness episodes happen en route. Upon arrival to ED, we tell them about the runs/episodes, they see the pads are on and we get a room real quick. ED MD walks in the room after hearing talk of vtach from my medic ( patient is awake and alert at this point, just nervous by all the hustle and bustle of her arrival just complaining of mild nausea ) told us we were overreacting to put pads on and that this was artifact. We straight up ask him, “those are aren’t runs of vtach?” He basically kinda blew us off saying that some things are artifact and blocks and pads weren’t necessary, and “if anything ‘pads’ view added to the artifact part” and moved on to talking to the patient right then and there, so obviously at that point it was time for the ol get-nurse-signatures-and-scram thing. My medics logic for pads is he thought she may need to be cardioverted if her presentation deteriorated further.
But anyway, I always love hearing what you guys think. I’m in paramedic school and I’m not gonna lie if I got this on a test I’d have no idea what to call this rhythm, it looks pretty vtach ish to me but there seem to be QRSs? Im unsure what I’d say for final answer. Thoughts ?
TL;DR ugly EKG; ED MD said artifact; thoughts on rhythm, what you’d do if you saw it in the field?
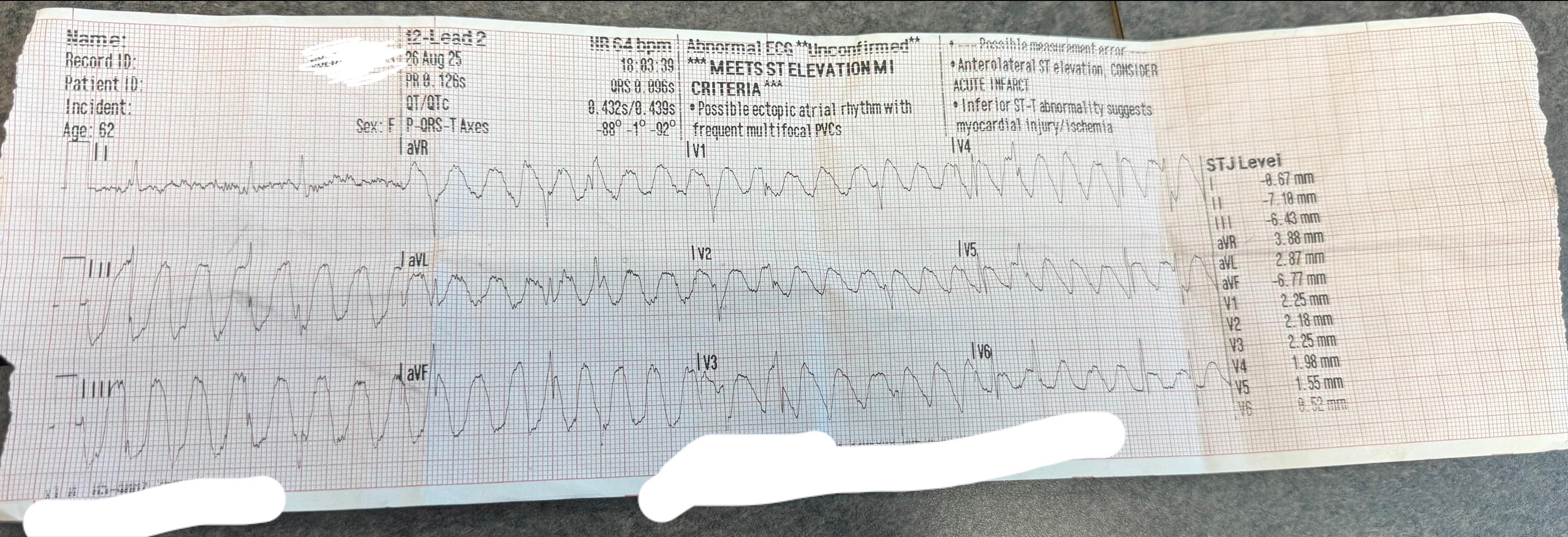
EDIT: SOLVED! Aslanger's sign - This phenomenon occurs due to tapping of arterial pulse on the ECG electrodes, which is known as arterial pulse tapping artifact. YES, THIS WAS ARTIFACT :) I learned my lesson - The patient's left (or right) leg electrode must've been placed on the posterior tibial artery causing artifact - this is why lead 1 looks normal. The pt was in afib and bradying down causing her intermittent loss of consciousness. I very much appreciate all comments on this post, they've helped me learn a lot.
The big squiggles are 100% artifact. Lead II is the key, because it shows clear narrow complex beats (probably slow A fib) with. You can't have VT everywhere except one lead.
I would also like to know what the patient's pulse was like during the unresponsive episodes, either from the pulse ox or palpation. She could definitely be having syncope from bradycardia.
this call really threw me for a loop im glad im not a medic yet to have had to make some sort of field impression on it. Any thoughts on what it possibly couldve been justed based on info given?
Look at lead I. This is definitely some sort of artefact. This is either AFib with slow ventr. resp. or brady with frequent SVES. The baseline would help for comparison. Did she have a tremor?
It sure sounds like it! I guess I let my medic convince me of one thing, and kinda tunnel visison'd past the real rhythm. I appreciate everyone in this thread giving me the reasons why we were incorrect in this situation, it really helps me learn.
Your precordial leads come from your limb leads. Wilson's central terminal is the specific name for the central point derived from the limb leads used for your precordial leads. Look up einhovens triangle and Wilson's central terminal to learn more on that all.
The higher the limb leads are placed (nearer the torso) the more likely there will be changes due to slight positional differences/movement, but the less likely there is to be artifact. For formal ECGs, guidelines are to place the electrodes distally on the wrists/ankles, and move them closer to the torso if there is any unavoidable artifact (e.g. due to tremor, a baby moving). If the leads are moved up, this should be noted on the ECG as it is not standard placement and it may affect analysis of different ECGs over time.
For EMS, as far as I know most people don't expect as accurate electrode placements, due to the likely high stress/sub-optimal conditions the ECG is performed under, and a "cleaner" ECG is more useful than one with heavy artifact in acute situations.
Have done EKGs for hospital patients. Some are emergency, including EKGs during rapid response calls. Tons of screamy moving patients. Babies and kids, people with Parkinson’s or agitated dementia, people with mania/psychosis (baseline for QT before antipsychotics), restless STEMI/OMI patients, intoxicated people, etc.
I get that not all patients are able to hold still and relax their arms/legs for 10 seconds. Still, it’s extremely rare that I’m not able to get a clean EKG with all electrodes placed in standard positions. Arm electrodes are for the arms, and leg electrodes are for the legs. Many people use Mason-Likar placement, but the EKG may be different compared to standard placement.
If you’re able to, I’d try to use standard placement. I wouldn’t immediately go to Mason-Likar placement if you can avoid it. You can use anywhere from shoulder to wrist for RA and LA, and anywhere from the hip to the ankle for RL and LL. I’ve always liked using the calves or thighs, and the arms or shoulders.
Anyway, remember that time goes from left to right over all leads. Imagine holding a pen vertically to the paper and moving it from left to right. Everything on the same vertical line happens at the same time. Lead I happens at the same time as leads II and III. Example of sinus rhythm below.
The biggest trick I know for removing baseline wander and motion artifact is to gently rub the skin with dry gauze before placing the stickers. Takes two seconds and can make the difference between a readable EKG and an unreadable EKG. Also, don’t use rubbing alcohol.
This is a classic case of tunnel vision. Big squigglys look scary! But let's break this down so you can learn and not let it happen again.
Understanding the anatomy of an EKG is so important. The EKG is broken up into 4 chronological sections. Think of them as columns that all occurred simultaneously. Lead I, II, III... aVR, aVL, aVF, V1-3 and V4-6. Each column of leads is recorded simultaneously, so you can compare the complexes to other complexes in that column, but not necessarily to another column because those occurred at a different time. So in this case compare Lead III to Lead I. Do the complexes match? No, not really. That should raise a red flag. Lead II to Lead I, ah, we see obvious hidden "buried" QRS complexes that do match if we could unburry them.
Since this patient presumably does not have two hearts, these leads which were captured at the same time showing different readings should lead you to the conclusion that there is a fault with the EKG tracing and should be investigated.
When every lead is impacted with a finding (in this case, high amplitude, low frequency) except a single limb lead which is spared, you can deduce that the finding is artifactual from one of the limb electrodes.
The options are right arm (RA), left arm (LA), left leg (LL). Right leg is the ground electrode. Lead I: LA - RA
Lead II: LL - RA
Lead III: LL - LA
Notice that in lead I, LL is absent from the equation. Similarly, LA is absent from lead II and RA is absent from lead III. Every other lead incorporates all three limb electrodes in the equation.
So, if the artifact spares lead I, it must be from the LL. If it spares lead II, it must be from the LA, and if it spares lead III, it must be from the RA.
Narrow complex beats are still visible, don’t have fusion morphology, and some are in the absolute refractory period of the preceding artifact “complex.”
I mean, as others have pointed out the big scary squiggles are artefact rather than VT, but I wouldn’t necessarily expect a paramedic to unpick that in the field, especially given the history of syncope. Bringing them as a priority call to the ED with pads on in case she lost consciousness again is totally reasonable.
But i find the fact that your medic thought it was v-tach coinciding with multiple lapses in consciousness and still was only going to cardiovert if she “deteriorated further”.
Nothing at all wrong with putting the pads on. I hope the doc treated it as a learning experience and wasn’t a dick about it. At first glance, that does look ugly. Only after you pick it apart does it look more like artifact and less like a bad day.
I wish we had a live chat to ask questions when Im 2 machines in and they can’t go any flatter and I just want to cry in memaws face. I have more to learn.
The artifact issue is well explained by other posters. Looking at the EKG I am wondering if we are seeing an effective / perfusing rate of @ 45 bpm; the R-R interval pattern seems to be consistently 120, then 60, then 120 … etc. I wonder if this is a bigeminal non-perfusing PAC contributing to the syncope? The leg shaking might not have been obvious but I wonder if it was a hypoxic tremor.
What was the pts position when found vs during transport? Ex was she laying in bed? I know we tend to default to semi-Fowlers for transport and for someone who’s just barely holding on to their hemodynamics that could have contributed as well.
Regardless, IMO it’s not unreasonable to throw pads on someone who appears to be unstable. The IV was more invasive.
Hey thank you so much for this comment! That article seems like it would be fascinating but it seems like you need a membership or something for further info.
Unfortunately, it is a subscription site. Inexpensive & well worth the money for emergency medicine folks wanting to exercise their emergency EKG muscle.
Edit/Follow up: Yes everybody! I hear ya loud and clear - this was indeed pulse tapping artifact or aslanger’s sign (not pattern). Very fascinating learning opportunity, thanks to everyone who commented
The loss of consciousness with that rhythm would have concerned me for sure. Always better to be prepared than not. If she had coded and the pads were already on then she gets defib faster.
This was simply all my medics thought process was, thank you for understanding. When we arrived and the doc seemed confused about pads, I was then also confused prompting my post to get others' thoughts on it lol. my lead 1 totally looks like afib, but the rest of it is just so ugly

{kind=link}
88
u/Yeti_MD 5d ago
The big squiggles are 100% artifact. Lead II is the key, because it shows clear narrow complex beats (probably slow A fib) with. You can't have VT everywhere except one lead.
I would also like to know what the patient's pulse was like during the unresponsive episodes, either from the pulse ox or palpation. She could definitely be having syncope from bradycardia.