r/Paramedics • u/[deleted] • 3d ago
US Here’s my personal EKG from two months ago. Guess what it was and you get an internet high five.
{kind=link}
If you nail
67
u/Bronzeshadow 3d ago
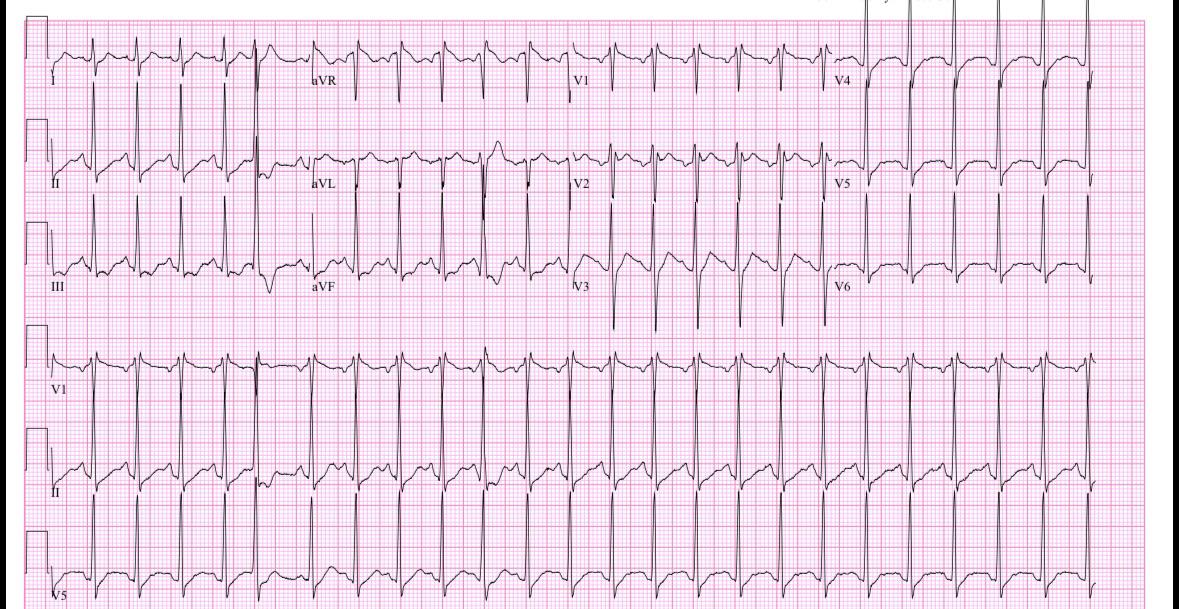
Holy Hypertrophy Batman. Those QRS's are so big they'll make an RN blush.
21
3d ago
Wild right! Echo came back totally normal!
13
u/LBBB1 3d ago edited 3d ago
Makes sense, I’m glad. There is no left ventricular strain pattern. High voltage can be normal in young adults or people with a thin/athletic build. This is why voltage criteria for LVH usually don’t apply to people below the age of 35 or so.
https://ecg-interpretation.blogspot.com/2013/08/ecg-interpretation-review-73-lvh.html?m=1
6
3d ago
Wow! Great catch and spot on
1
u/joeymittens Physician Assistant (PA-S2), Paramedic 15h ago
Are you a thin individual? Sometimes it looks like hypertrophy, when in reality it’s just a thin person with not much tissue to read through. So if appears like large QRS complexes
2
u/Bronzeshadow 3d ago
Waaaaaaaaaaah?!? Alright I'll put my thinking cap half on because it's late and I'm not nearly as drunk as I want to be. Narrow complex @ about 150 or so. P waves look a bit inverted but they're present and uniform so Afib is out. Finally answer SVT. Then again there's that one R-R that's goofy but it's mostly uniform? Fuck it i'd push adenosine and figure it out from there.
11
1
u/bacongas 2d ago
Kind of would like to know how this pt presents before I pushed adenosine. I’ve seen people vagal out of this by trying to blow the plunger out of a syringe. How was OP looking and feeling is my question and I’m too lazy to read any further down. Some kind of SVT. How far away is the hospital? ABCs? Airway, Breathing, Can you walk to the stretcher?
22
u/TovarichBravo 3d ago
This is what happens when you have way too much caffeine and virtually no potassium. Guaranteed.
Hope you were actually seen for this and didn't just take an EKG at work and let it ride.
13
3d ago
You’re exactly right, and oh I was admitted for a day, absolutely
10
u/TovarichBravo 3d ago
Trade out those energy drinks for something that replaced electrolytes. Not sugarade or other bullshit red dye 40 flavored syrups. try LMNT or something similar. Keep hydrated. Kick the caffeine addiction and you'll be surprised how much better you sleep and how little it takes to get up in the morning 💪
5
3d ago
Yeah definitely! I switched to coconut water for the last two months, I feel pretty good overall!
2
u/un_cereal 3d ago
Hey, can you explain what clued you in that OP was hypokalemic?
3
u/TovarichBravo 3d ago
U waves, tall P waves, and what appears to be ST depression in a few spots that don't make sense for an MI. I can't see the measurements but it seems wide for being so fast, that's also another red flag for me.
14
12
u/rads2riches 3d ago
Inappropriate sinus tach: no discernible etiology or vagal issues.
Appropriate sinus tach: shitty diet, stress
5
3
3
u/lemonsandlimes111 3d ago
lol this was me two months ago, me and my partner both did this on our new lifepak 35 to test out how to do the 12 lead from our normal lifepak 15s. Both had hypertrophy and were like this is broken, 15s read it the same for both us. We’re both 26 🤣
1
2
2
3d ago
Answer: HYPOKALEMIA/STRESS
Two Bolus of potassium and 10 hours later my EKG returned to normal..
2
u/Wenckebach2theFuture 3d ago
Hypokalemia shouldn’t cause sinus tach. Could have been stress. But also could have been atrial tach, p wave morphology looks similar to a sinus p wave, so if AT would like be a crista AT.
1
3d ago
One would think right? Lol I guess that’s why we call it practicing medicine. New things everyday
1
u/Helassaid 3d ago
A gram or two of caffeine might.
1
u/Wenckebach2theFuture 2d ago
Sure, amongst other arrhythmias too. But if the rate is fixed in place without much variation, should suspect AT.
2
u/harinonfireagain 3d ago
4 Red Bulls, tones dropped, and you’re in the can - I just don’t know why you’re running a twelve lead
2
2
2
u/throdoswaggins 2d ago
Emt b here. You definitely have a heart beat. I'm gonna call for ALS backup.
2
u/Cyborg-drone-8914 2d ago
SVT with a ton of ischemia I’d say? I’m assuming the rate is too fast to fully perfuse the heart, leading to global ischemia as seen with the numerous ST depressions or something
1
1
u/12345678dude 3d ago
Myocarditis or a PE?
2
3d ago
D-Dimer tested negative, so nope!
1
1
1
1
1
3d ago
Hint - it’s extremely simple
1
u/deadaimer 3d ago
Sinus tach with lvh
1
3d ago
Sinus tach absolutely, but no LVH. Understate guess because of the QRS complex. But the echo came back with the heart structurally normal.
1
1
1
1
u/Imaginary-Emu-2693 3d ago
too much caffeine !
1
3d ago
I wish that was the case😂
1
u/Imaginary-Emu-2693 3d ago
aw man, maybe panicking or running?!
1
1
1
1
1
u/ImNotABot-BEEPBOOP 3d ago
s1q3t3 … right heart strain. you said d-dimer was negative so not likely pe, pneumonia, heavy exercise, pneumothorax, or major trauma. my guess is volume or oxygen depletion. anemia or dehydration?
1
1
1
1
1
1
u/Due-Peach-1876 3d ago
Looks like you’re fine. Maybe you should try drinking more water and being less of a female dog.
1
1
1
u/throdoswaggins 2d ago
Emt b here. You definitely have a heart beat. I'm gonna call for ALS backup.
1
1
u/SpicyPropofologist 2d ago
Also looks like RBBB. Maybe rate dependent? Do you know if your anteroseptal leads have the RSR' pattern at slower rates as well?
3
u/LBBB1 2d ago edited 2d ago
My guess is that the incomplete RBBB isn’t real. It’s from high V1/V2 misplacement. Negative sinus P waves in V1 and V2. Have seen many EKGs with this pattern become normal with standard placement of V1 and V2.
https://litfl.com/misplacement-of-v1-and-v2/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8293594/figure/anec12844-fig-0001/
3
3
u/SpicyPropofologist 2d ago
So, in a properly placed v1 & v2, they sit inferior to the SA node, so the subsequent electrical pathway to the AVN would be towards the properly placed leads, producing a positive (or possibly biphasic) P wave? Because it's negative, though, I can safely discount the RSR' pattern? Or is that overly simplistic? Thank you for the link, BTW. I see a lot of EKGs / strips, and continue to learn as much as I can. Still sometimes a challenge!
1
u/LBBB1 2d ago
That’s exactly it. The sinus P wave is positive when moving towards a lead, and negative when moving away. V1 is placed over the right atrium. It doesn’t make sense for the sinus impulse to move entirely away from V1. This only happens when V1 is placed too high, or when the heart is shifted downwards in severe COPD (extremely hyperinflated lungs). I don’t know of any other causes. Unless the patient has severe COPD, a negative sinus P wave in V1 means that V1 was placed far too high. Very common.
I’m not convinced that the incomplete RBBB pattern means anything. It doesn’t look like a real incomplete RBBB to me. It actually looks like a very specific pattern that is seen with high V1 placement. It’s very easy to give someone this type of pattern with high V1 placement.
1
1
u/WeAudiHere 1d ago
What was your PR interval? Looks very close to WPW. PR appears to be right below .12 but also the image isn’t great quality so it could be right at it. Though, I wouldn’t consider that a prominent delta wave.
1
49
u/Due-Order2153 3d ago
I enjoy interpreting fast sinus tachycardia like this. People will argue that a rate above xxx is SVT, but one of the discriminators for SVT is a lack of discernable P wave which is clearly present. The T Wave isn't super sharp so that tends to place the Atrial Flutter in the probably not category.
Did you have an epinephrine dump from some sort of adrenal problem?